Imagine your body’s foundation, your bones, gradually losing their inherent strength, becoming soft and pliable instead of robust and rigid. This concerning condition, medically known as osteomalacia, directly translates to "soft bones." Unlike the more commonly recognized osteoporosis, which involves a thinning of bone tissue, osteomalacia is fundamentally a problem with bone mineralization – the process by which newly formed bone tissue hardens into its strong, mature form. While various factors can contribute, the primary culprit behind this debilitating disorder is often a profound vitamin D deficiency, hindering the body's ability to absorb essential minerals like calcium and phosphate.
This article will delve into the intricacies of osteomalacia, exploring its mechanisms, diverse causes, tell-tale symptoms, and the crucial steps towards diagnosis and effective treatment. Understanding osteomalacia is key to preventing its progression and restoring vital bone health.
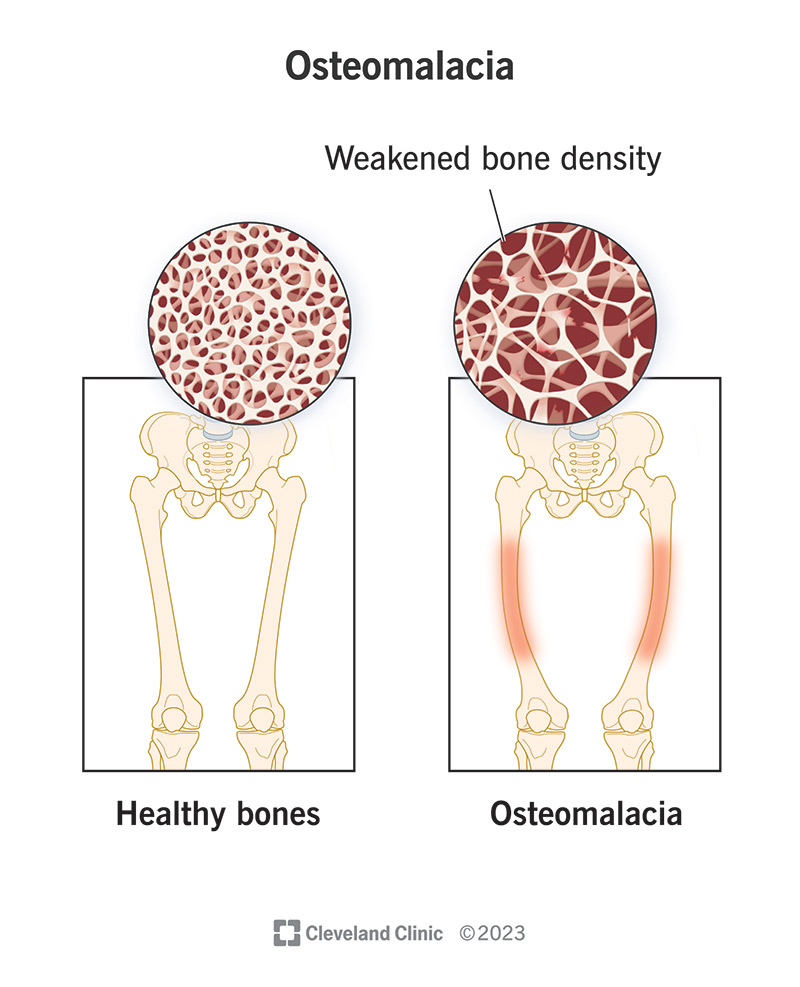
Understanding Osteomalacia: More Than Just Soft Bones
At its core, osteomalacia is a metabolic bone disorder where the bone matrix, the organic framework upon which minerals are deposited, fails to adequately mineralize. Think of it like a building where the concrete hasn't properly set, leaving the structure weak and prone to damage. In healthy bones, calcium and phosphate are precisely laid down within this matrix, giving bones their characteristic hardness and resilience. When this process falters, often due to insufficient vitamin D, the bones remain soft and weakened.
It's important to differentiate osteomalacia from a related condition, rickets. While both involve inadequate bone mineralization, rickets affects children whose growth plates are still open, leading to growth abnormalities and skeletal deformities. Osteomalacia, however, primarily impacts adults after growth plates have fused. Consequently, it doesn't alter bone length but significantly increases bone fragility, leading to a higher risk of bending, fractures, and persistent discomfort. For a deeper dive into how this condition stands apart, you can explore the nuances in Osteomalacia vs. Osteoporosis: Key Differences in Bone Health.
The consequences of unmineralized bones are profound. They become less capable of bearing weight, making everyday activities painful and increasing vulnerability to what are known as pathological fractures – breaks that occur with little or no trauma, simply because the bone can no longer withstand normal stresses.
The Root Causes: Why Bones Lose Their Hardness
The etiologies behind osteomalacia are varied, but a central theme revolves around inadequate mineral availability or impaired mineral metabolism. Identifying the specific cause is paramount for successful treatment.
The Pervasive Role of Vitamin D Deficiency
Vitamin D is not just a vitamin; it's a prohormone crucial for calcium and phosphate absorption in the intestines. Without sufficient vitamin D, even an adequate dietary intake of these minerals won't reach the bones effectively. The primary reasons for vitamin D deficiency include:
- Insufficient Sunlight Exposure: Our skin synthesizes vitamin D upon exposure to ultraviolet B (UVB) radiation. Factors like living in higher latitudes, spending most time indoors, using excessive sunscreen, or wearing extensive clothing can severely limit this natural production. Individuals with darker skin pigmentation also face a higher risk, as increased melanin acts as a natural sunscreen, reducing vitamin D synthesis.
- Dietary Inadequacy: While some foods are fortified with vitamin D (e.g., milk, cereals), and fatty fish naturally contain it, many diets fall short of recommended intake.
- Malabsorption Disorders: Conditions that impair nutrient absorption in the gut can lead to vitamin D deficiency regardless of intake or sun exposure. These include celiac disease, Crohn's disease, cystic fibrosis, and states following bariatric surgery, which alter the digestive tract.
Other Significant Etiologies
Beyond vitamin D, several other factors can disrupt mineral balance and lead to osteomalacia:
- Phosphate Deficiency: Phosphate is another critical component of bone mineralization. Deficiencies can arise from rare renal tubular disorders that cause excessive urinary phosphate loss, or from prolonged use of certain medications like aluminum-containing antacids that bind phosphate in the gut.
- Hypocalcemia (Low Calcium): While often linked to vitamin D deficiency, hypocalcemia can also stem from parathyroid gland dysfunction, as the parathyroid hormones play a vital role in regulating calcium levels.
- Certain Medications: Some drugs interfere with vitamin D metabolism or mineral absorption. Anticonvulsants like phenytoin, used for epilepsy, can accelerate vitamin D breakdown in the liver.
- Rare Oncogenic Osteomalacia: In very rare cases, tumors, usually benign, can secrete a hormone called fibroblast growth factor 23 (FGF23). Elevated FGF23 levels inhibit phosphate reabsorption in the kidneys and suppress vitamin D activation, leading to severe phosphate wasting and osteomalacia.
Key Risk Factors
Several groups are at a higher risk of developing osteomalacia:
- Elderly Individuals: The skin's ability to synthesize vitamin D diminishes with age, and older adults often have reduced sun exposure.
- Darker Skin Pigmentation: Higher melanin levels reduce UV light penetration, limiting vitamin D synthesis.
- Obesity: Vitamin D is fat-soluble and can be sequestered in adipose tissue, reducing its bioavailability in the bloodstream.
- Individuals with Malabsorption Syndromes: As mentioned, conditions affecting gut absorption are significant risk factors.
- Residents of Regions with Limited Sunlight: Geographical location plays a role, especially during winter months.
- Long-term use of certain medications: Particularly anticonvulsants or medications affecting mineral absorption.
The global prevalence of osteomalacia is likely underestimated, with postmortem studies in certain populations indicating it could affect up to 25% of individuals, highlighting its widespread, yet often silent, impact.
Recognizing the Signs: Symptoms of Osteomalacia
The symptoms of osteomalacia often develop gradually and can be subtle, leading to misdiagnosis or delayed treatment. They frequently mimic those of other musculoskeletal conditions, making accurate identification challenging.
- Diffuse Bone Pain: This is one of the most common and debilitating symptoms. Patients often describe a deep, dull ache that can be constant and worsen with activity or weight-bearing. It typically affects the lower back, pelvis, hips, thighs, and ribs. The pain is not relieved by rest and can become quite severe.
- Proximal Muscle Weakness: Weakness in muscles closest to the body's center, particularly in the legs and shoulders, is another hallmark. This can manifest as difficulty rising from a seated position, climbing stairs, or lifting objects. A characteristic "waddling gait" may develop due to hip muscle weakness, increasing the risk of falls.
- Bone Fragility and Fractures: As bones soften, they become highly susceptible to fractures from minimal trauma. These are often referred to as pathological fractures. In some cases, imaging may reveal "pseudofractures" or Looser's zones – incomplete fractures that appear as linear areas of demineralization, commonly found in the femur, pelvis, or ribs.
- Associated Hypocalcemia Symptoms: If vitamin D deficiency is severe enough to cause significant hypocalcemia (low blood calcium), patients may experience secondary symptoms such as muscle cramps, numbness or tingling sensations (paresthesia), and in severe instances, tetany (involuntary muscle spasms).
- Fatigue: Generalized fatigue is a common complaint, often stemming from the overall metabolic imbalance and chronic pain associated with the condition.
Because these symptoms can be non-specific, a high index of suspicion is required, especially in individuals with known risk factors.
Diagnosing Osteomalacia: The Path to Clarity
Accurate diagnosis of osteomalacia requires a comprehensive approach, integrating clinical findings with laboratory tests and imaging studies.
- Clinical Evaluation: A thorough medical history focusing on dietary habits, sun exposure, medication use, and any pre-existing conditions (e.g., malabsorption) is crucial. A physical examination may reveal bone tenderness, muscle weakness, or a waddling gait.
- Laboratory Tests: Blood work is often highly indicative:
- 25-hydroxyvitamin D (25(OH)D): Levels are typically low, often below 20 ng/mL, and can be severely deficient (<10 ng/mL).
- Calcium: May be low (hypocalcemia) or at the lower end of the normal range.
- Phosphate: Often low (hypophosphatemia).
- Alkaline Phosphatase (ALP): Usually elevated, indicating increased bone turnover as the body tries to compensate for the poor mineralization.
- Parathyroid Hormone (PTH): Often elevated in response to low calcium and vitamin D levels, a condition known as secondary hyperparathyroidism.
- Imaging Studies:
- X-rays: Can reveal characteristic pseudofractures (Looser's zones), particularly in the pelvis, femur, and ribs. Generalized bone demineralization may also be visible.
- Dual-energy X-ray Absorptiometry (DEXA) Scan: While DEXA scans show reduced bone mineral density (BMD), which is common in osteomalacia, this finding is not specific to the condition and can also be seen in osteoporosis. It helps assess overall bone health but usually requires additional tests for a definitive osteomalacia diagnosis.
- Bone Biopsy: In cases where the diagnosis remains ambiguous, a bone biopsy, typically taken from the iliac crest, is considered the gold standard. It directly visualizes the bone tissue, revealing characteristic widened osteoid seams – layers of unmineralized bone matrix – confirming the presence of osteomalacia.
Treating Osteomalacia: Restoring Bone Strength
The cornerstone of osteomalacia treatment is to address the underlying cause, primarily by correcting vitamin D, calcium, or phosphate deficiencies and promoting bone remineralization. With appropriate intervention, most cases of osteomalacia can be effectively managed, leading to significant improvement in symptoms and bone strength.
For a comprehensive guide on managing this condition, delve into Osteomalacia Explained: Causes, Symptoms, and Soft Bone Solutions, which offers detailed insights into the available treatments and long-term care strategies.
Correcting Nutritional Deficiencies
The primary therapeutic approach involves high-dose supplementation:
- Vitamin D Supplementation: Patients usually require substantial doses of vitamin D, often in the form of ergocalciferol (D2) or cholecalciferol (D3), to rapidly replenish stores. Initial doses can be very high, followed by maintenance doses once levels normalize. The specific regimen depends on the severity of the deficiency and the patient's individual response.
- Calcium and Phosphate Supplementation: Along with vitamin D, calcium supplements are typically prescribed, especially if dietary intake is insufficient or if hypocalcemia is present. Phosphate supplementation may also be necessary in cases of severe phosphate wasting.
Addressing Underlying Causes
Beyond supplementation, it's crucial to manage the specific etiology:
- Malabsorption Syndromes: Treatment involves managing the primary gut disorder (e.g., gluten-free diet for celiac disease, anti-inflammatory medications for Crohn's) alongside higher doses of vitamin D and minerals, often administered via intramuscular injections or specialized formulations to bypass intestinal malabsorption.
- Renal Tubular Disorders: Management focuses on correcting electrolyte imbalances and reducing phosphate loss, often requiring specialized nephrological care.
- Oncogenic Osteomalacia: Surgical removal of the tumor responsible for secreting FGF23 is the definitive treatment. If surgery isn't feasible, medications that block FGF23 activity may be used.
- Medication Review: If certain medications are contributing to the problem, alternatives may be considered, or careful monitoring and increased supplementation may be necessary under medical supervision.
Practical Tips for Bone Health
Beyond prescribed treatments, integrating healthy habits is essential for long-term bone health and prevention:
- Embrace Safe Sun Exposure: Aim for 10-30 minutes of direct midday sun exposure (without sunscreen) several times a week, depending on skin type, location, and season. However, always prioritize skin cancer prevention.
- Diversify Your Diet: Incorporate vitamin D-rich foods like fatty fish (salmon, mackerel, tuna), fortified milk, orange juice, and cereals. Calcium-rich foods include dairy products, leafy greens (kale, spinach), and fortified plant milks.
- Regular Weight-Bearing Exercise: Activities like walking, jogging, and strength training help stimulate bone formation and improve overall bone density.
- Stay Informed and Consult Professionals: If you have risk factors or experience symptoms, don't self-diagnose. Consult your doctor for appropriate testing and a tailored treatment plan. Regular monitoring of vitamin D and mineral levels is key to preventing recurrence.
The goal of treatment is not only to alleviate pain and prevent fractures but also to restore normal bone mineralization and improve muscle strength, allowing individuals to regain their quality of life.
Conclusion
Osteomalacia, the softening of bones due to inadequate mineralization, is a significant metabolic bone disorder primarily driven by vitamin D deficiency. While its symptoms can be subtle and easily confused with other conditions, understanding its unique impact on adult bones—leading to increased fragility, chronic pain, and muscle weakness—is critical. Early diagnosis through a combination of clinical assessment, blood tests, and imaging, followed by targeted treatment, typically involving high-dose vitamin D and mineral supplementation, can effectively reverse the condition and restore bone strength. Proactive measures such as adequate sun exposure, a nutrient-rich diet, and regular medical check-ups, especially for those at risk, are vital in safeguarding bone health and preventing the debilitating effects of osteomalacia.